I am trying to run a binary classification problem on people with diabetes and non-diabetes.
For labeling my datasets, I followed a simple rule. If a person has T2DM in his medical records, we label him as positive cases (diabetes) and if he doesn't have T2DM, we label him as Non-T2DM.
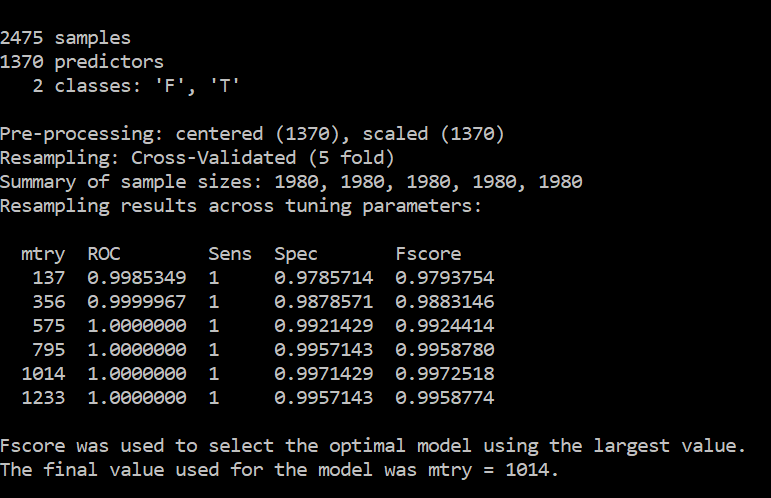
Since there are a lot of data points for each subject, meaning he has a lot of lab measurements, a lot of drugs taken, a lot of diagnoses recorded, etc, I end up with 1370 features for each patient.
In my training, I have 2475 patients and in my testing, I have 2475 patients. (I already tried 70:30. Now am trying 50:50 still the same result (as 70:30))
My results are too good to be true as shown below
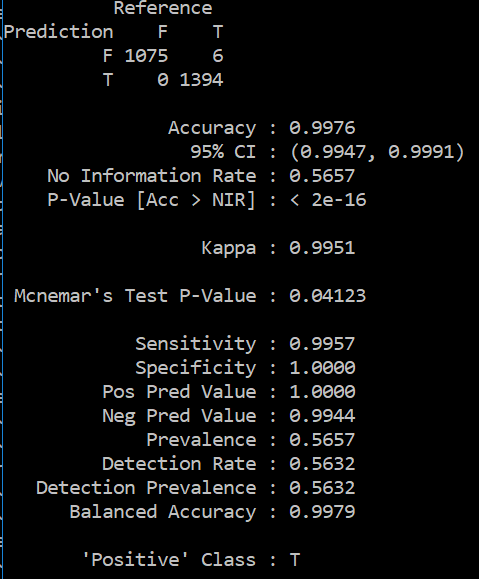
Should I reduce the number of features? Is it overfitting? Should I retain only the top features like top 20 features, top 10 features etc? can help me understand why is this happening?
Detailed Update
We check for the presence of T2DM by a set of diagnosis codes (like icd9,10 codes for T2DM and its complications etc). For ex: let's say if a patient has an icd9 code of 250 in his diagnosis records, we know that he was diagnosed with Type 2 diabetes. Let's not worry about the accuracy of this labeling approach at this point. Similarly, we label all other patients as T2DM and Non-T2DM.
But when we extract features, all his medical records are treated as features. The frequency of the drug/condition/lab tests will be used as a feature value. So, basically, the same diagnosis code (250) will be an input feature as well. Does it mean I should drop the diagnosis codes which were used to label a dataset from being used as features? But those are really very good features that can help me find out whether a patient is diagnosed with T2DM or not (when I apply my model on a totally different dataset). My objective is not to find out whether a patient will develop diabetes in the future or not but my objective is only to find out whether a patient is diabetic or not (from his records). So, I label my dataset with an imperfect heuristic as stated above and build a model. Once I build this model, I would like to validate this model at another site and find out how good is the model built using this imperfect heuristic in identifying whether a patient is diabetic or not. Hope this helps